
This is a read for anyone who has had gaps in their sex education, who does not quite understand their own body and how it works, or how their partner/s body works. This read is about the biology, and the pleasure of our bodies.
 Sometimes when we talk about matters of sex, people may have different ideas of the definitions of words. So to kick things off from the outset. Let’s be clear…
Sometimes when we talk about matters of sex, people may have different ideas of the definitions of words. So to kick things off from the outset. Let’s be clear…
A person’s sex is biologically determined (what you are born with), and Gender is a social construct. So when I say ‘male’ or ‘female’ I am referring to a person’s biological sex and NOT their gender identity. A little more on that shortly.
This presentation will cover the following areas:
Sexual Anatomy of D.S.D. /Intersex bodied people.
Sexual Anatomy of Females.
Biology of Sexual Response of Females.
Sexual Anatomy of Males.
Biology of Sexual Response of Males.
* WARNING* In this document there are images of anatomy and biology which are very detailed and graphic.
Let’s begin.
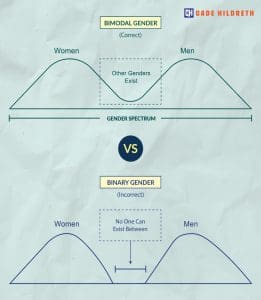
Image @cadehealth
A person’s Sex (what they are born with) can be male, D.S.D. (also known as Intersex), and female. The sex is biologically determined.
D.S.D. is an umbrella term used to describe a variety of bodies whose characteristics, whether physical, chromosomal or hormonal, do not conform to female or male. Intersex people are “I” in LGBTQIA+.
There are around 40 different conditions that affect the development of sexual and reproductive organs in utero. Consequently the variations of what a person is born with inside and on the body is quite diverse.
Many countries around the world on birth certificates only recognise Male and Female, and have historically encouraged a limited amount of time to ‘determine whether a person is Male of Female’. Many babies and children have had to unnecessarily undergo corrective surgery which unfortunately for many D.S.D. people has been very traumatic.
D.S.D. is becoming more accepted and recognised at birth in countries such as Germany and Kenya.
Emily Nagoski beautifully repeats the phrase ‘all the same parts, organised in different ways’ in her book Come as you are. Gonads are ovaries in females, and testes in males. In foetus development, it isn’t until the 8th week that the gonads develop turning into either male testes, or female ovaries (or both as a possibility for D.S.D. bodied people).
To branch off in to being female or male comes down to chromosomes. Females have XX, Males have XY.
The SRY gene influences the bipotential of gonadal development. It Is most always on the Y chromosome, and is responsible for development of testes. Not having a Y chromosome means that there won’t be any SRY, so the default development will be ovarian. For many people development of their gonads isn’t complete.
The SRY gene is what kicks off a whole lot of processes that are steps in further development. The ovaries or testes go on to develop hormones. When ovaries or testes fail to develop completely, it has implications in later development during teenage and adult years including the ability to reproduce.
Sexual (external) Anatomy of Intersex Bodied People- Some variations.

Image @vielma.art
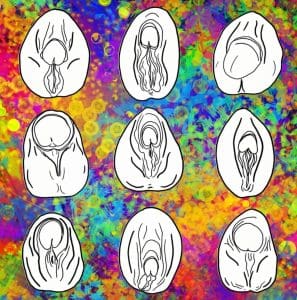
Image @vielma.art
Here are just a few examples of some variations of what a D.S.D. person’s genitalia might look like. The sexual anatomy inside the body can have many variations too. So to clarify, a person can be born with the biological sex of Female, D.S.D., and Male. Soon as we look at the Sexual anatomy of females and males, you will see just how similar they are. Like Natalie Nagoski says “Same parts, organised in different ways.”
Sexual Anatomy of Females

Image @gynodiversity
To be honest when looking at the anatomy for the female sex, there are quite a lot of parts and systems involved. Let’s start with what we can see on the outside (all of which can be referred to as the vulva- yes what you can see here from the front and under view in these pictures are all vulvas).
In Female Sexual Anatomy, we are going to be looking at all the different parts related to sex including: The Vulva, Anus, Clitoris, Vagina, Pelvic Floor Muscles and the Reproductive System. We will also look at some changes to the vulva and vagina during Menopause.
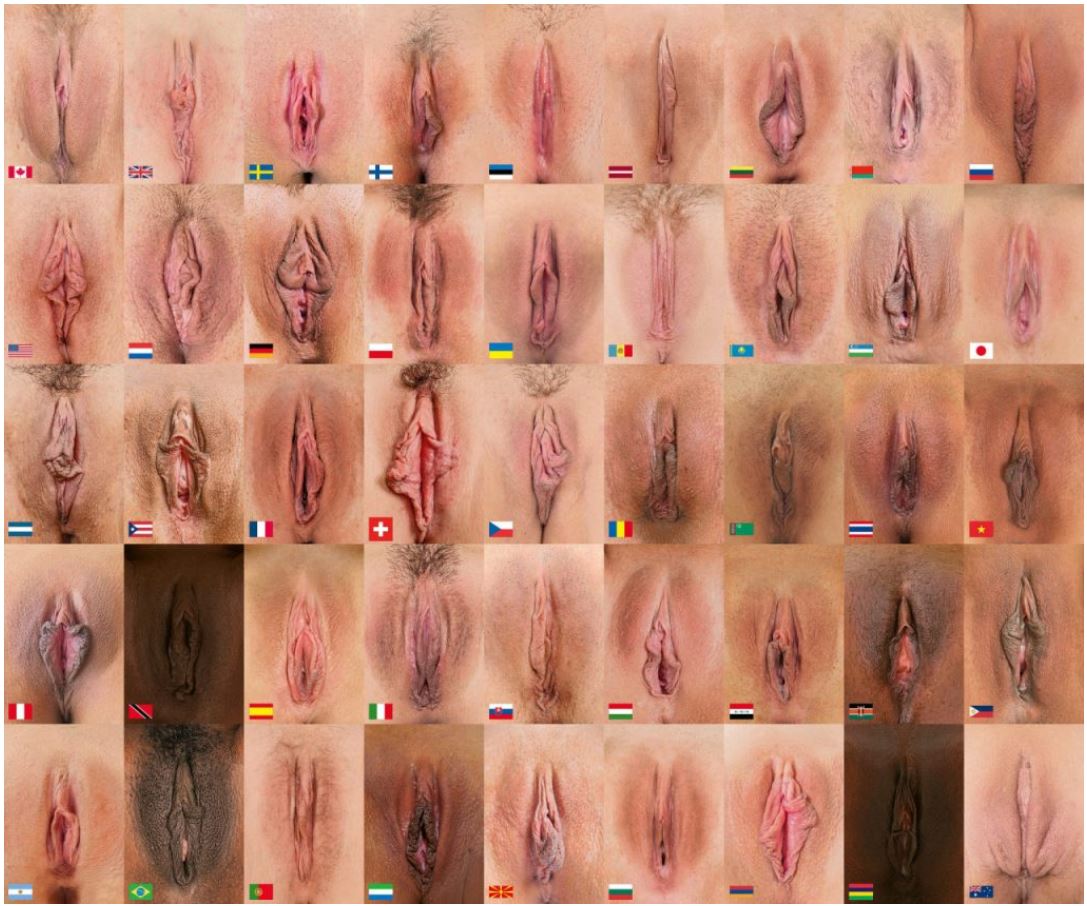
Generations of females globally have had negative associations with their genitals whether it be from cultural shame, pain, due to many years of patriarchal oppression both socially and medically. This still exists today. Many Female bodied people carry shame and mystery as to how their own bodies work which affects their access to pleasure and health. Take a good look as these vulvas of the world of different ages. Let’s demystify what female sexual anatomy is and what it does. Female sexual anatomy is a part of the body worth celebrating with its ability to give life and produce pleasure.
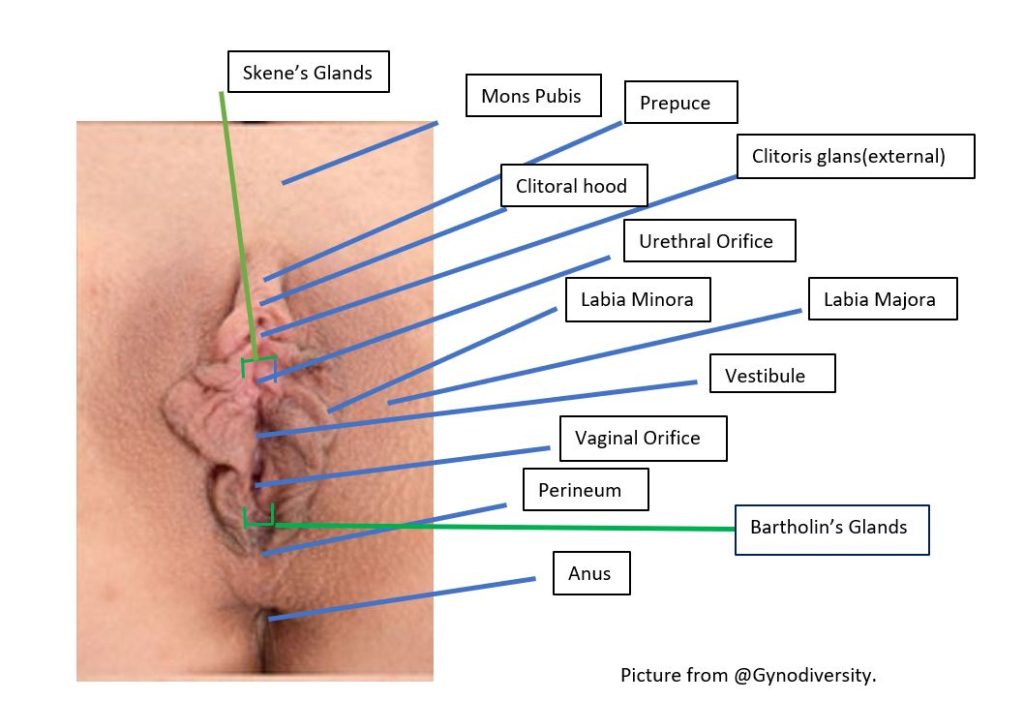
This picture is of a vulva without pubic hair. Vulvas are highly individual in their visual appearance with many parts being variable in the size and colours. Pubic hair is also variable in density often growing on the Mons and Labia majora ,and can grow on the inside of the upper legs near the vulva and around the anus.
Mons Pubis and Labia Majora– Soft and fatty thought to provide protection for more sensitive areas. The skin is however still sensitive to touch and irritations.
Prepuce/Clitoral Hood– Skin that provides some protection for the sensitivity of the external part of the clitoris.
Clitoris– Only a small amount is visible externally. Internally it is quite extensive in size, and all parts of the clitoris are made from erectile tissue and is pleasurable. More on the clitoris later.
Urethral Orifice– Where urine leaves the body. Very small hole.
Labia minora– Is sensitive non fatty skin protecting the external part of the clitoris that when moved around can stimulate the clitoris. It is also comprised of erectile tissue. When the female body is aroused, the labia minora swells with blood becoming more ‘open’ on both sides of the inner part of the vulva where it attaches to the vestibule. The labia minora unite over the glans clitoris to form the clitoral prepuce otherwise known as the clitoral hood. Many people have a distorted perception of what ‘normal’ labia minora ‘should’ look like. Media and pornography where images have been manipulated favouring a small tucked in labia minora, have contributed to many females feeling that they are abnormal. If their labia minora protrude past the labia majora, some females seek labiaplasty (surgically removing part of the labia minora). This can reduce sexual pleasure. In FGM, some cultural practices involve removal of part or all of the labia minora, labia majora and sometimes the external part of the clitoris. Painful complications from this can arise and sexual pleasure can be compromised. However due to the fact that the clitoris is quite large internally, sexual pleasure and orgasm is still possible.
Vestibule-The area of the vaginal and urinary openings along with the glands.
Vaginal orifice– Can be partially covered by a thin skin called the hymen (not pictured) that is usually torn through exercise or penetration. The vaginal orifice is the beginning of the birth canal that is a fibromuscular tube surrounded by pelvic connective tissue on all sides. The function of the vagina is to facilitate childbirth, menstruation and to act as the receptacle for the penis during PIV sexual intercourse. It is also rich in nerve endings (particularly at the entrance) which is a sensitive and pleasurable area for exploration in sexual play, and in penetration if desired. The vagina is also one of the most expansive organs of the female body due to the extensive connective tissue space surrounding the vagina which results in the expansion of the vagina during childbirth. It heals quickly post birth, and is self-cleaning.
Perineum– sensitive area located between the Vaginal orifice and the anus.
Bartholin’s Glands– Two pea sized glands situated just inside the opening of the vagina which are similar to the bulbourethral glands in males. These glands secrete mucus that lubricate the vagina.
Pubic hair- (not shown in this picture) Is thought to provide some padding, hold scent from sweat and oils which is musky with pheromones. Gentle tugging of hair pulling the skin of the mons and the labia majora is also pleasurable.
Anus– Has two sphincters the internal and external. Rich with nerve endings in its lining. Many nerves account for it being a place for stimulation and pleasure in sexual play for many people. The anus is not self-lubricating. Due to its rich blood supply and delicate skin, it is easy to contract an STI in sexual play with a partner/s. Use of lubrication and Safe sex practices are necessary.

Helen O’Connell unknown photographer
Helen O’Connell Australia’s first female urological surgeon. Frustrated by the medical texts she studied in the 1980’s when they did not have any description of the clitoris in them (when there was a whole chapter on the mechanism of a penile erection). Much attention was given to preserving sexual function during surgical procedures on men, yet in women it seemed incidental. At the time there was no available manual on the nerves and blood supply to the clitoris. Dr. O’Connell studied many cadavers, and used magnetic resonance imaging to map the clitoris, showing that it was made from erectile tissue and that the vestibular bulbs are a part of the clitoris. Also that the urethra and vagina are closely related structures that form a tissue cluster with the clitoris which is the site of female sexual function and orgasm. She succeeded in showing a 3D simulation of a clitoris and it’s 15,000 nerve endings in the pelvis.

Ciltoris 3D Model. Unknown Image Source.

Image @PeterThmark
On the left we can see a 3D printed model of the clitoris thanks to Dr O’Connell. It is this part on the upper tip which is visible on the outside of the body, the rest is internal. I like this picture as you get a sense that it is not flat as is often drawn in diagrams. Parts of the clitoris reach deep inside the body. The image on the right shows the clitoris superimposed in where its position lies in relation to the vulva. As all parts of the clitoris are sensitive, this is good to know for mapping pleasure in Sexual play.
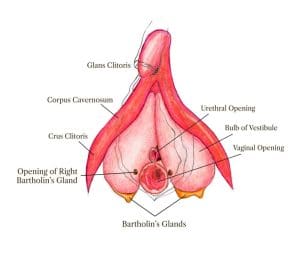
Image @CICS
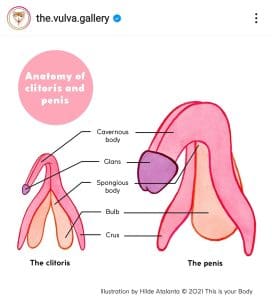
Image @the.vulva.gallery
The Clitoris built for pleasure. It has a pair of corpora cavernosa enclosed in dense fibrous tissue which fills with blood to make the clitoris grow in size when stimulated. Similar to the penis, yet the clitoris doesn’t have a urinary function.
All parts are erectile.
All parts are pleasurable.
Its clitoral bulbs sit either side of the vagina roughly underneath the area of the labia majora and around the urethra, and when erect the grow in size and are responsible for pressure against the wall of the vagina which makes the vaginal canal feel snug. This is also why penetration at the entrance of the vagina can feel pleasurable.
When the clitoris is stimulated, the part of the brain which is activated overlaps with the part of the brain that lights up during nipple stimulation. Interestingly this the part of the brain that also has cross over with the nerve pathways to the uterus. Hence why breast feeding can stimulate the uterus to contract. Nipple stimulation in sexual play has implications for increasing pleasure in the clitoris, even when the clitoris has been damaged or partially removed.
As the connections between the clitoris, urethra and vagina are complex, many people like to call it the clitoro-urethro-vaginal complex or simply the clitoro complex. More on that bit later!

Image @SamWebster
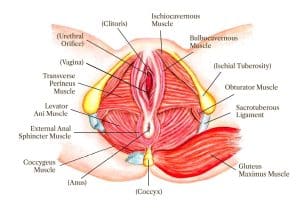
Image @CICS
The Pelvic Floor is made up of the muscles, ligaments, nerves and tissue that sit at the base of the pelvis. It attaches to the pubic bone at the front all the way through to the tailbone at the back. It is often described as acting like a sheath or sling to support the pelvic organs – the bladder, bowels and reproductive organs but also assists in the continence of the bladder, bowel, sexual function as well as trunk stability and mobility.
In orgasm they contract 3-15times.
If the muscles are too weak it can lead to prolapse, if they are too tight they can lead to sexual or pelvic pain.
Exercises to strengthen the pelvic floor for appropriate tonality and promote blood supply to it and the surrounding tissue is healthy.
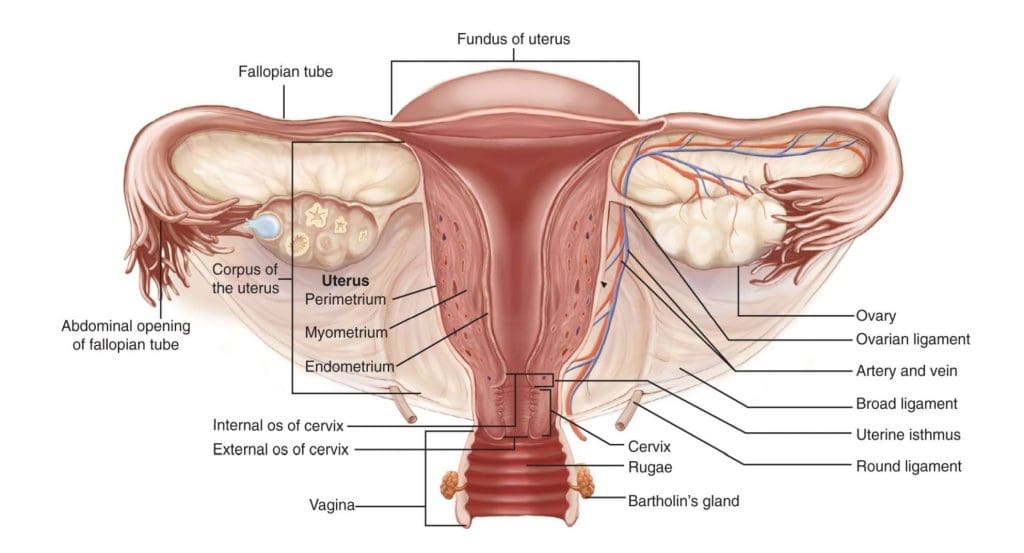
Image @CICS
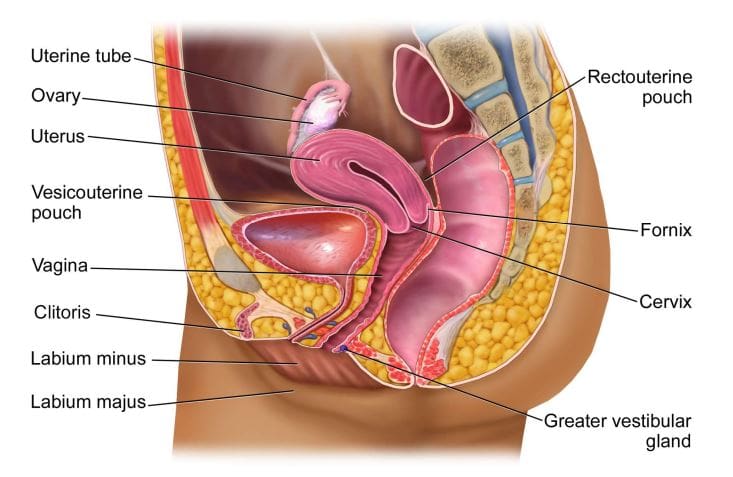
Image @CICS
Skene’s Glands– Similar to the male prostate secrete PSA. PSA is found in ‘female squirting’ approx. 1-2 mL. (more on that later too).
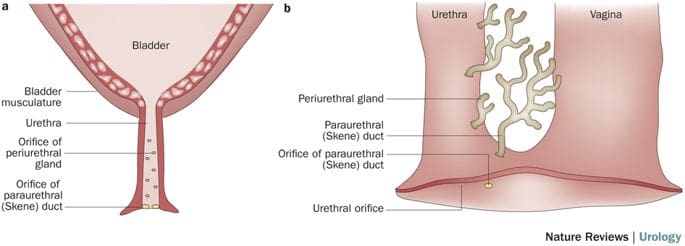
Image @NatureReviews
The vaginal Canal is a passage that is surround by smooth muscle that can contract involuntarily. This muscle is well supplied with many blood vessels that can aid speedy rejuvenation if it is injured.
Length of the vagina is variable in individuals. The length of the vagina gets longer when a female is stimulated.
Vaginal dryness is a very common problem. Although often associated with the menopause (it affects more than half of women after the menopause), it is also very common for women to experience it at other times of their lives and there are many contributing factors resulting in vaginal dryness including:
- Endocrine therapy
- Breastfeeding
- Normal monthly cycle
- Anxiety
- Side effect of medication
- Surgery
- Dermatological conditions
- Sjogren’s Syndrome
- Diet and lifestyle choices
- Sex reassignment surgery
The vaginal canal– is wet.. The lining of the vagina is made from tissue which allows for wetness to pass from the internal body into the vaginal canal. Upon stimulation more mucus is created and lubricates the vaginal canal in preparation for penetration to lessen friction and microtears.
If microtears happen, the cells inside the vaginal walls grow quickly repairing the tears every 96 hours.
It is a clever self-cleaning part of the body shedding old cells and keeping healthy bacteria with a pH of 4.5. It discharges around 1-4 ml daily which it’s consistency, appearance, smell and taste can change depending on the menstrual cycle. During menstruation the pH slightly increases.
Uterus- Also known as the womb has 4 sections. Cervix. Corpus (main body). Fundus (top section) Uterine Isthmus (thin part at the bottom above the cervix).
Walls of Uterus- Have a tough outer layer, muscular inside that contracts, and inner layer which is rich in blood vessels. This is the part that gets thicker each month on the influence of hormones in preparation for conception and pregnancy, and is discharged in menstruation if a pregnancy does not occur.
Fallopian tubes- 8-14 cm and muscular and guide eggs (ova) released from the Ovaries into the uterus.
Ovaries- Produce Oestrogen, Progesterone and Testosterone. Each month they take turns to release an ova at the point of ovulation.
Menstrual cycle- 21-35 days hormones guide the release of a single ova from the ovaries for possible conception. The endometrium gradually thickens on the inner walls of the uterus to nourish the possible fertilised ova. If it is not fertilised, the lining is released in the form of Menstruation. The Uterus contracts to help this process.
Menstruation also known as a period is the shedding of blood and tissue from the uterus that lasts 4-6 days. It can be painful, and cause females to be iron deficient.
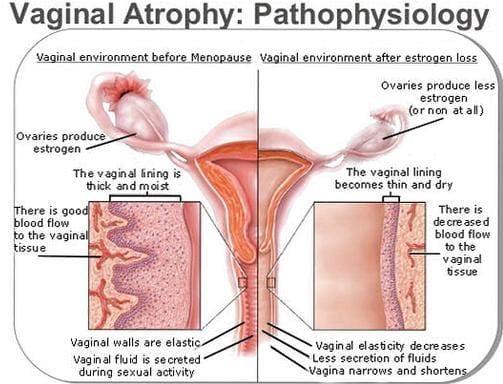
Image unknown source
Menopause Is when a female no longer fertile (no period for 12 months), and it can be sudden resulting from some medical interventions. During menopause there is a decline in the bodies oestrogen and progesterone. This change can result in the tissues in the vagina and surrounding area become thinner and dryer, known as Vulvovaginal Atrophy (VVA). This symptom is experienced by 60% of peri and post-menopausal women. After menopause the cell lining gets 2/3 thinner in the wall of the vagina and the PH increases. There Less blood flow to pelvic area at this time. This dryness can result in daily discomfort, itchiness, burning and result in pain during intimacy or smear tests.
HRT (Hormone Replacement Therapy) has been helpful for many females as it reduces the symptoms of menopause. Females have also found that a daily yoga practice, exercise and arousal helps to increase blood flow to the pelvic region. A good quality lubrication which does not irritate the vagina or vulva is also helpful.
Studies show that approximately 50% of post-menopausal women will experience VVA related symptoms, such as:
- Vaginal dryness
- Irritation
- Painful intercourse (Dyspareunia)
- Trouble with urination
- Inflamed tissues
Many women will spend up to 40% of their lives in the postmenopausal stage.
Approximately 55% women going through menopause don’t seek counselling or do anything at all to treat symptoms.
Biology of the Female Sexual Response.

Image @oaknarrow
Theories of how females respond sexually have changed over time and are different in different cultures.
Masters and Johnson- Holds criticism for not addressing desire as an important component for arousal.
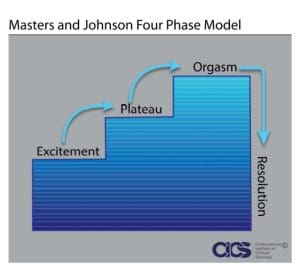
Image @CICS
Kaplan’s Model- Introduced the Psychological and Physiological phases, also holds criticism for being male centric by design as it fails to address intimacy as a desire that many females initially need.
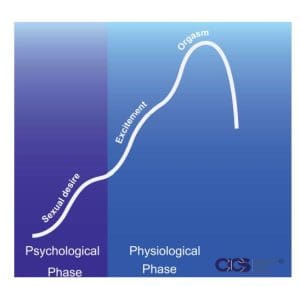
Image @CICS
Basson’s Model– Addresses the point that some females require intimacy to fuel motivation in response to sexual stimulus.
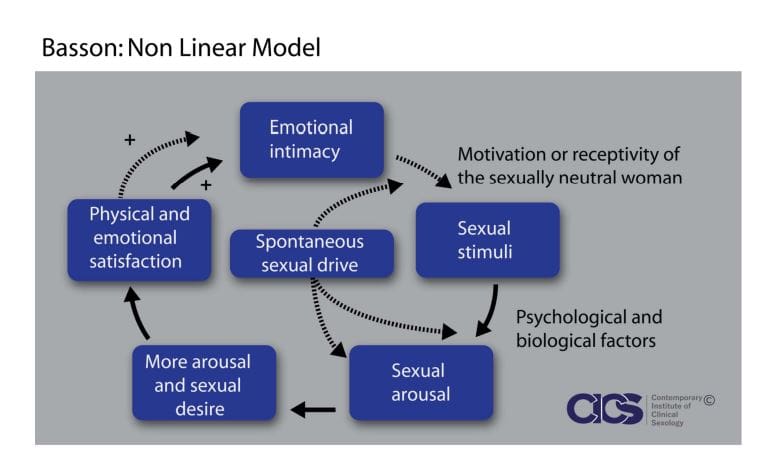
Image @CICS
Grand Master Taoist Mantak Chia- Presents a 4 phase model specific to females explaining the cultivation of sexual energy starting with arousal leading to multiple orgasms. This model suggests that when experiencing organism, females need to actively do the ‘upward draw’ Taoist technique while practicing mindfulness to then open the further chance of stronger successive orgasms. There is a spiritual dimension to this model. This model has been taught and practiced in Taoism for hundreds of years.
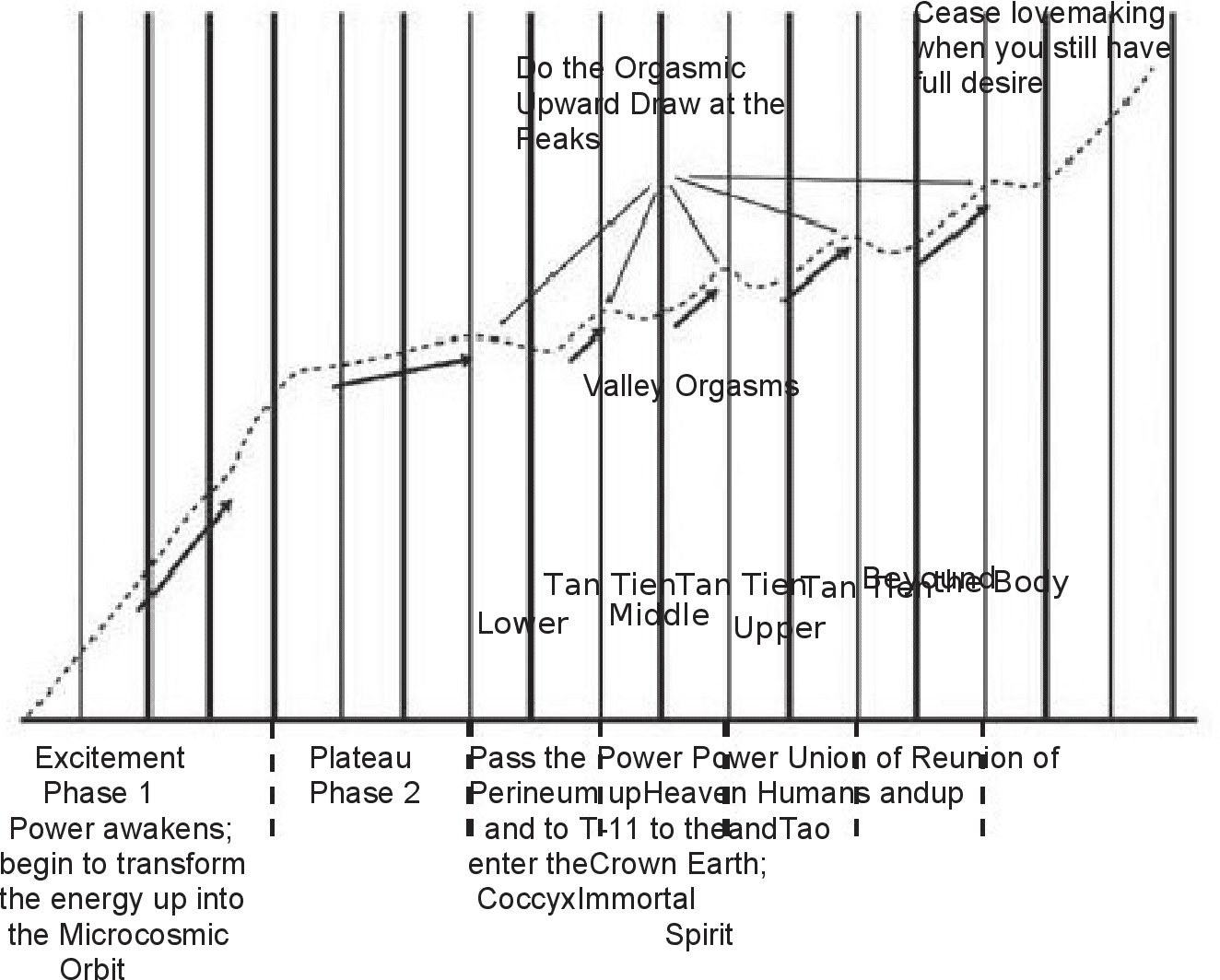
Image @MantakChia
There are many other models that exist, this is just a selection of a few. What would your own version of your sexual response model look like if you drew it? If you are sexual with another person, what would their model look like?
Desire in females can be both mental AND physical but not necessarily experienced at the same time. The mental is emotional and cognitive, and the physical is physical stimulation.

Image @almestal
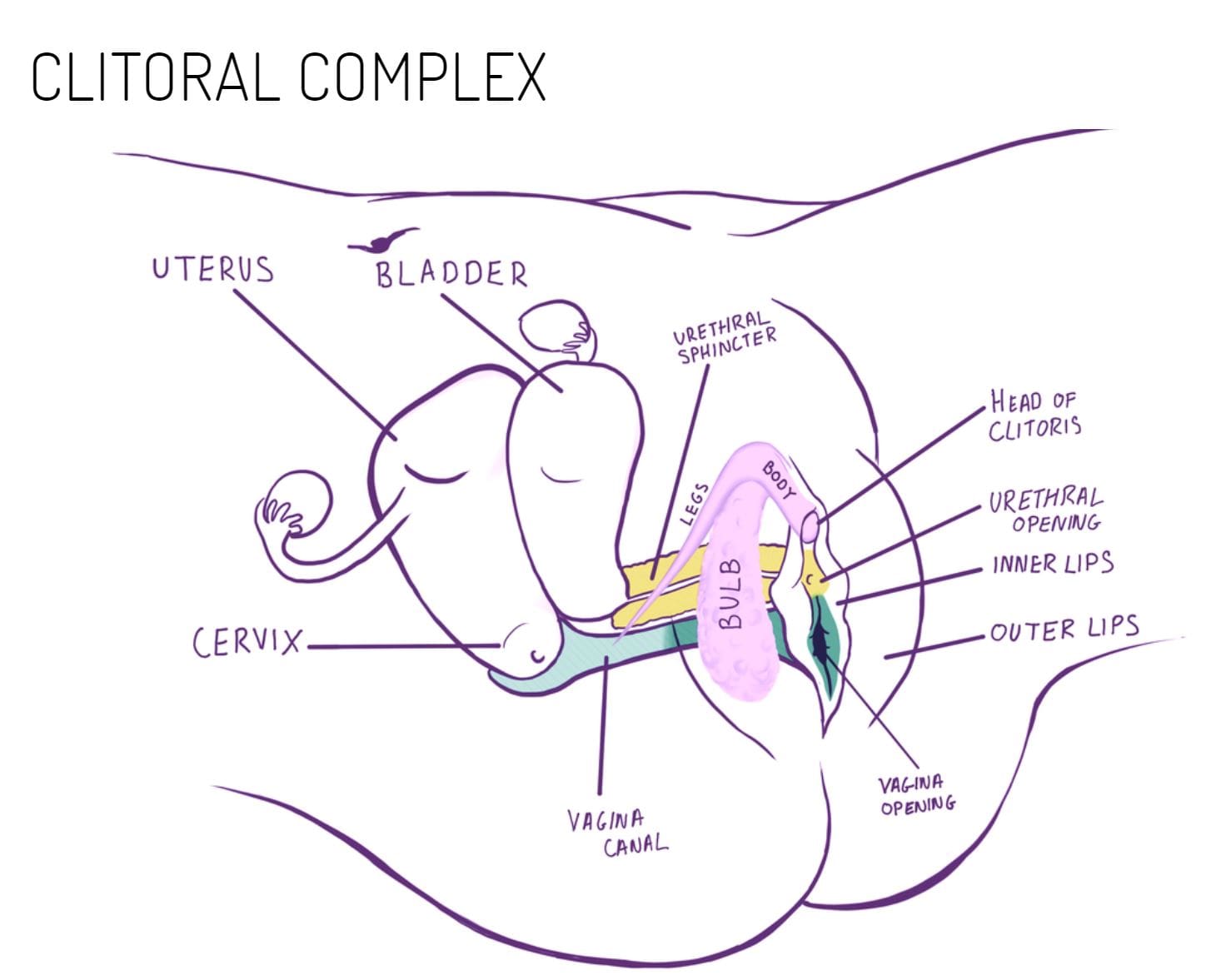
Image @anatomyofpleasure
Desire is the wanting of more activity that can lead to orgasm. The physiology of arousal characteristics are that:
There is increased blood flow to the vagina and surrounding area causing the vagina, clitoris and vagina to swell. The vaginal walls get darker from the increased blood flow and there is an increase in transudate (lubrication) of the vagina. The Batholin’s glans also release a small amount of lubrication. The clitoris becomes larger and more sensitive. The uterus lifts up. Nipples become erect and the breasts swell. Breathing, heartrate and blood pressure increases. There can be muscle spasms in the feet, hands and face. The muscles in the body can become more tense.
Contractions of orgasms can last 5-60 seconds and are rhythmic with contractions of between 3-15. Post-menopausal contractions in duration and intensity for many females can be milder. Oxytocin is released with the female feeling bonded and relaxed.
Females don’t have a refractory period, therefore it is possible to have multiple orgasms.
Post stimulation, the clitoris decreases in size, the uterus descends, the vagina shortens and the labia resume it’s ‘resting’ colour and shape as the sympathetic nerves resume control.
Only 25-33% of females are capable of achieving orgasm when penetrated alone. Most females require clitoral stimulation in various ways either in solo or partnered sex. Each female is different in what they find stimulating and requires exploration. Many females feel disconnected from their bodies and do not know how to access pleasure. Some females orgasm with pressure applied to the sensitive anterior wall of the vagina which stimulates the clitoris, urethra and skene’s glands. It has been called the G spot, but actually it is still stimulating the clitoris from inside the vagina. The area is better known as the clitoral complex.
Some females are known to ejaculate during stimulation which does not necessarily coincide with an orgasm. This is also known as Squirting. The skenes glands release approx. 1-2mL of PSA or “ejaculate” (in men it is about 5mL) mixed with other fluid. Mostly, the liquid ejaculated is shown to be liquid that has been released from the bladder that contains traces of urine. However, reports indicate that the scent is not of urine and can have a sweet taste. This is has references to cultural cross over with the ancient Greeks referring to the “Nectar of the Gods.” In Taoism it is referred to as the “second water gate” that opens. Western medical science is still learning about the female body.
Many females find it pleasurable to have the anus stimulated superficially and through penetration in solo or partnered sex. The anus is rich in nerve endings and blood supply.

Image @emirshiro
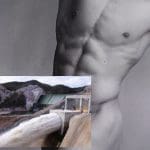
Image @emirshiro
Non-concordance is experienced by females and less so in males. Non-concordance can be experienced in two ways. It can happen for example when a person having a sexual experience has been mentally aroused, and the physical body has not responded, or the opposite where the body has responded to a sexual stimulus and the mind has not been aroused.
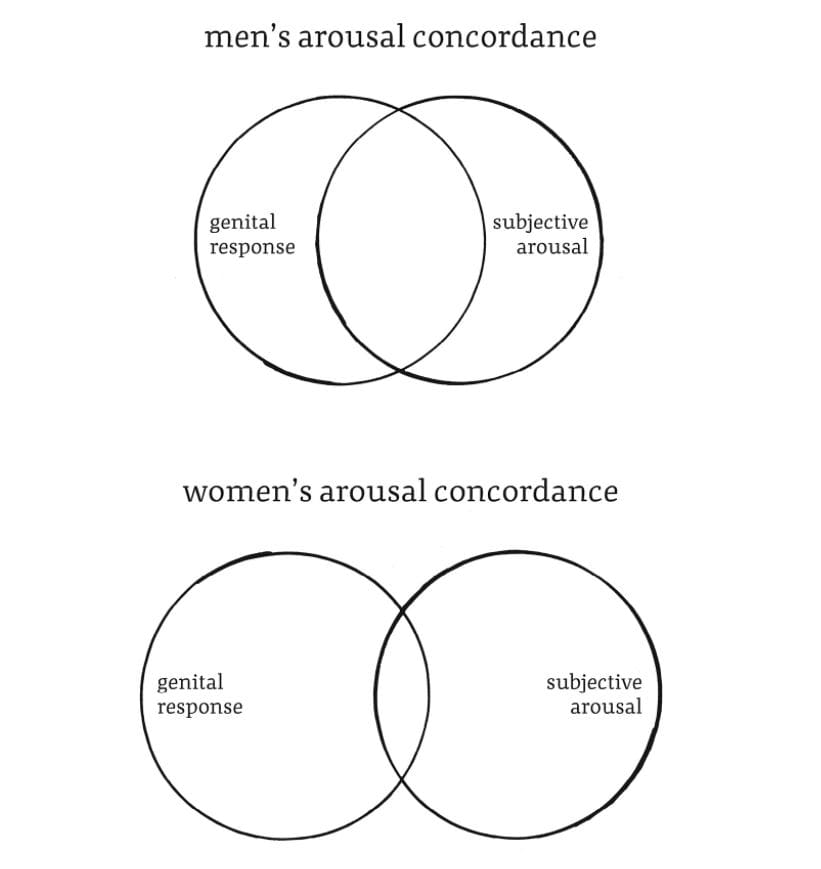
Image @EmilyNagoski
In female orgasm the Sacrospinal reflex with cortical control (L1, L2 sympathetic)- arousal and orgasms can happen without conscious control. Technically orgasms can happen involuntarily as a bodily response. Some Females who have been sexually assaulted have experienced orgasms which for the survivor, has been confusing and upsetting when they have not known this fact. Similarly if this happens in a sexual assault, the perpetrator not knowing this information may incorrectly and shockingly presume that the survivor has enjoyed being raped (?!?)
Sexual Anatomy of Males

Image @jaimiemccartney

Image @LauraDodsworth
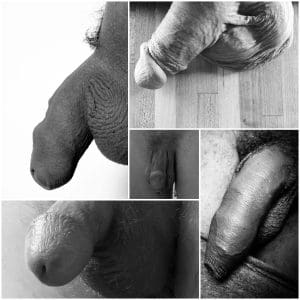
Image @LauraDodsworth
There is also much diversity in males. The amount of pubic hair, size and shape of the penis and scrotum, and whether or not the penis has been circumcised or not. There is a growing amount of males who are also self-conscious of the appearance of their gentiles and seek surgery for aesthetic changes.
Both the penis and scrotum are sensitive areas of the body and a space of pleasure when stimulated.
Penis size during an erection is variable in length and girth. Average stretched penile length of an adult male is approx. 12.5 cm +/- 2.7 cm. The average girth at the base of the penis during an erection is 12.1 cm.
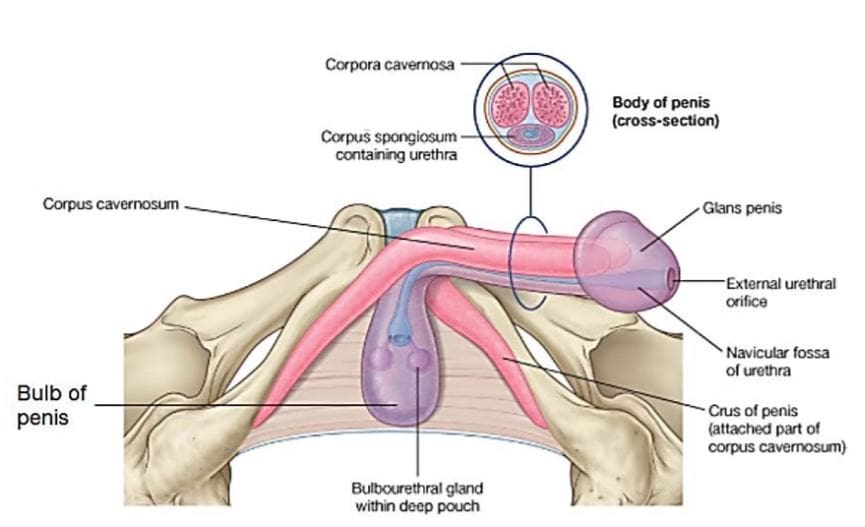
Image source unknown
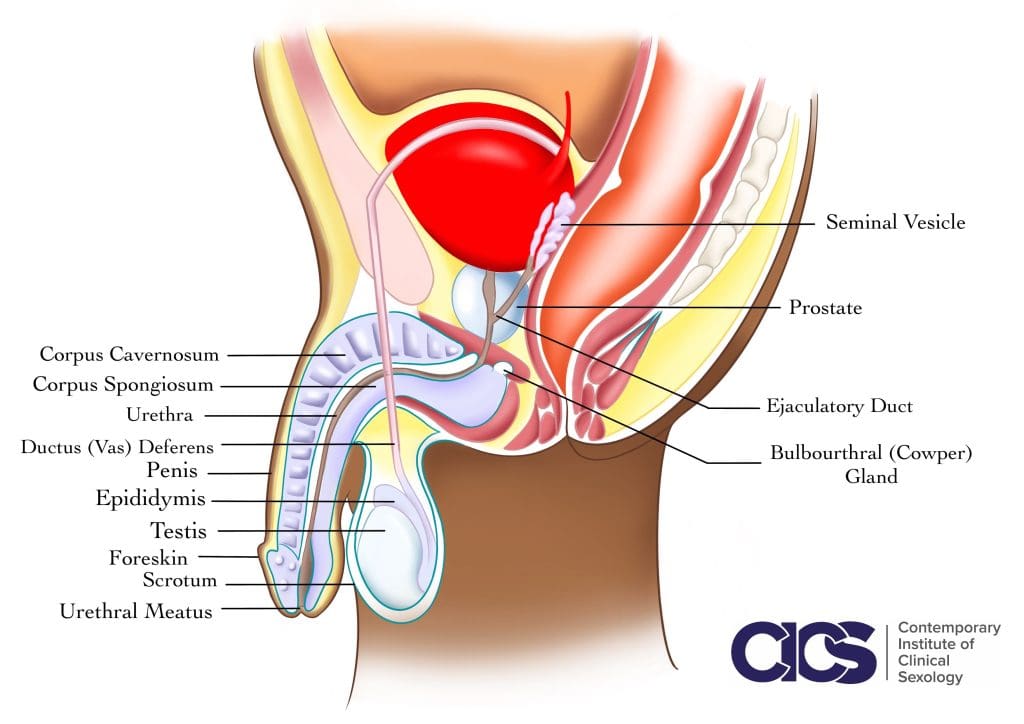
Image @CICS
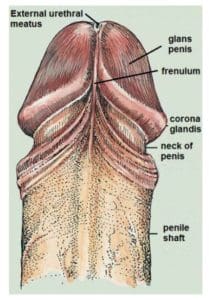
Image source unknown
The Penis mostly is external with internal parts. The internal root it is made up the bulb and the crura (or crus), the body of the penis is made up of the paired corpus cavernosum and the corpus spongiosum as well as the glans. The function of the Penis is for reproduction, and for urination.
The scrotum houses the male gonads called testes, the epididymis and the distal part of the spermatic cord.
The Corpora Cavernosa and the Corpus Spongiosum are erectile tissue which fills with blood in an erection (more about that later).
The testes make both testosterone which is the primary male sex hormone, as well as making sperm. The sperm is created in the seminiferous tubules before passing through the Epididymis.
The Epididymis both houses immature sperm until mature, and transports sperm by contraction into the vas deferens.
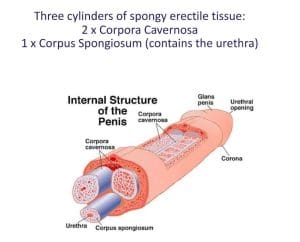
Image @CICS
The vas deferens is a muscular tube that starts in the testes at the epididymis into the pelvis up around the bladder and joins the urethra. It is the transport pathway of sperm to the urethra.
The Urethra is the tube which allows urine and sperm to move outside of the body.
The Seminal vesicles also known as the seminal glands secrete a fructose- rich alkaline fluid which the sperm use as an energy source and a coating agent that is mixed with sperm as it passes through the ejaculatory ducts. The secretions from the seminal vesicles makes up around about seventy percent of the volume of ejaculate.
The Ejaculatory ducts is the point of union of the vas deferens and seminal vesicles that empty into the urethra.
The prostate gland forms secretions which are important for sperm mobility. The secretions make up around 30 % of ejaculate. The prostate gland feels pleasurable when stimulated. It can be accessed through anal play, or through a particular pressure point located in the perineum which is referred to as the Million Dollar Point in Taoism.
The bulbourethral glands also known as the Cowper’s glands secrete a clear watery fluid that lubricates and repairs the urethra for the passage of sperm.
The Pelvic floor is a series of muscles in the pelvis that provides support to the organs and contract during orgasm, emission and expulsion of semen in ejaculation.
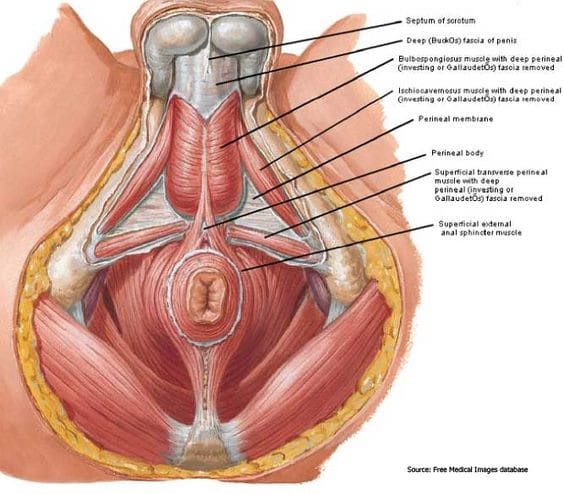
Image @rechargetherapy
Because of their attachments to the pelvis and hips, the pelvic floor muscles are an important part of the “core”. These muscles assist other abdominal, hip and back muscles to control movement of the sacroiliac and hip joints.
During intercourse, the pelvic floor muscles help to achieve and sustain an erection and allow for support during penetration. Sufficient strength of the pelvic floor muscles is necessary for orgasm, and excessive tension or sensitivity of the pelvic floor can also contribute to pain during or after intercourse.
Many factors can weaken pelvic floor muscles, including the surgical removal of the prostate (radical prostatectomy) and conditions such as diabetes and an overactive bladder. This can lead to urinary or faecal incontinence or dribbling after urination.
The Anus is full of nerve endings and is rich in blood vessels. The rich nerve endings make it sensitive so you can differentiate and control the passing of air and faecal matter. It is also a pleasurable when stimulated, particularly as it is closely located to the prostate. It is possible for males to orgasm from anal penetration.
It is not self-lubricating, and STI transmission is highest in anal sex due to the delicate tissues and blood supply. Barrier protection and lubrication is essential.
Biology of the Male Sexual Response
Image @emirshiro
Image @CICS
The model on the left shows 4 phases from a male being aroused through to orgasming and ejaculation that was created by Masters and Johnson. It implies that males are capable of one orgasm and does not mention when ejaculation happens.
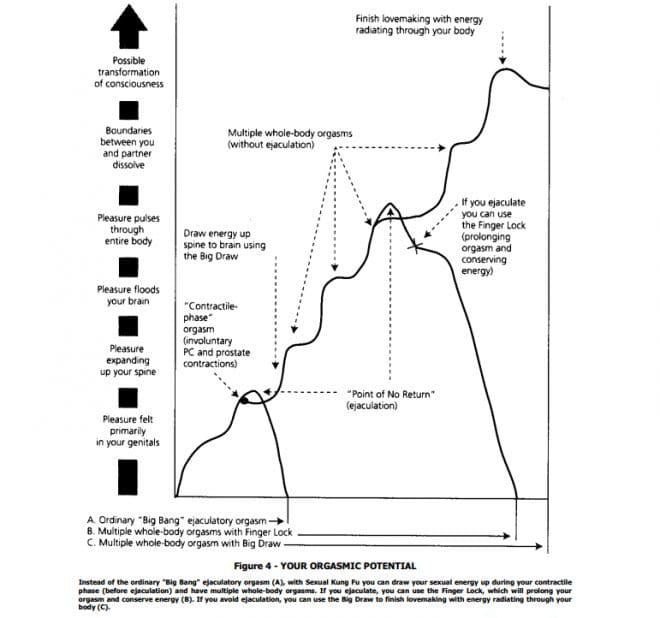
Image @MantakChia
This is a Taoist model a few hundred years old. It implies that males can have multiple orgasms, and orgasms do not necessarily have to coincide with ejaculation. It also suggests a spiritual element.
Different cultures have varied views on the process of what happens during male sexual arousal and their capabilities.
Sexual arousal and stimulation exits in both the mind and the body.
Sexual Stimulation and touch sensation provide the impulses that are delivered to the spinal cord and to the brain.
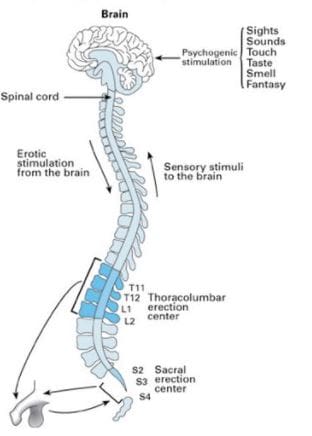
Image @humansexualitytoday
Reflex Erections are an automatic reflex response which do not involve erotic thoughts, or imagery in the brain. This reflex reaction is controlled by the spinal cord between T12- S3. The regular flushing of blood to the penis is thought to keep it healthy (more on this later).
Erections can also happen when the mind is stimulated from having pleasurable thoughts, imagery, sounds and exposure to scents and tastes. Erections also happen by stimulation from touch in different parts of the body that are pleasurable. These are erogenous zones and are quite individual.
The brain can both amplify sexual arousal and can equally inhibit it. Thoughts can act as being both an accelerator and a break in the level of stimulation. A busy mind will inhibit an erection.
How male erections happen
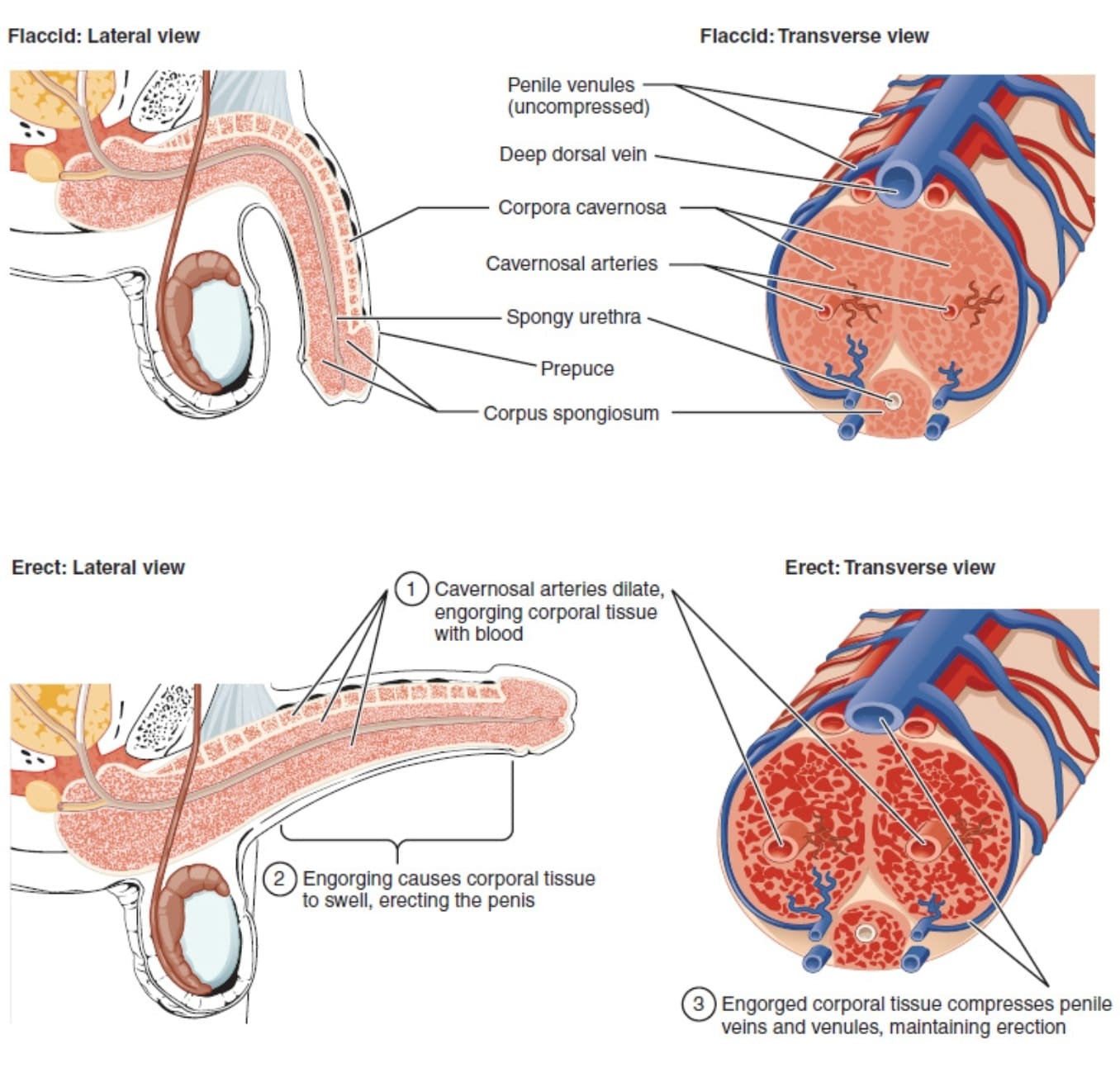
Image unknown source
We learnt earlier that erections can happen when aroused in the mind or though physical stimulation. Erections can also happen involuntarily when a male is not aroused. It is thought that involuntary erections happen naturally (particularly during sleep) so there is a regular robust flushing of blood into the tissue to keep it healthy.
During arousal the brain sends signals to start a hormonal response triggering the blood flow to increase to the penis. Blood goes into the arteries filing up the corpora cavernosa, and as the penis gets bigger it constricts the veins which are on the outer side of the penis trapping the blood inside causing an erection.
The penis returns to its flaccid state when the brain stops sending signals and there is a cessation of a hormonal response.
Erectile dysfunctions occur when:
- The brain doesn’t send the right signals to the penis. ( e.g. in Alzheimer’s and Parkinson’s).
- The blood flow is inadequate to the penis. (High blood pressure, heart disease, high cholesterol). Erectile dysfunction is a strong precursor to heart disease and should be investigated.
- Erectile tissue is damaged. (Pyronines disease, radiation treatment, diabetes, injury).
- Low Testosterone.
- Prostate cancer.
- Performance anxiety- When the male is feeling mentally under pressure..
When a penis is flaccid, it is kept that way when the sympathetic nerves are engaged. If you think about it makes sense, from an evolutionary perspective when males were hunting or escaping from being hunted, an erection would have been distracting. It is only when in rest and the parasympathetic nerves engage may an erection happen.
When the Parasympathetic nervous response engages, it allows for the release of Nitric Oxide that then triggers the release of an enzyme called cGMP. This allows for the smooth arterial muscles to relax and allows for increased blood flow to make the penis erect.
When a penis goes back to a flaccid state, the cGMP starts to break down which means that the smooth arterial muscles begin to tense back up causing the blood flow in the penis to reduce.
When males take a PDE5 inhibitor (such as Viagra) to assist with maintaining an erection, the PDE5 is inhibiting the body to breakdown the cGMP which results in maintaining an erection for a longer period of time.
Ejaculation.
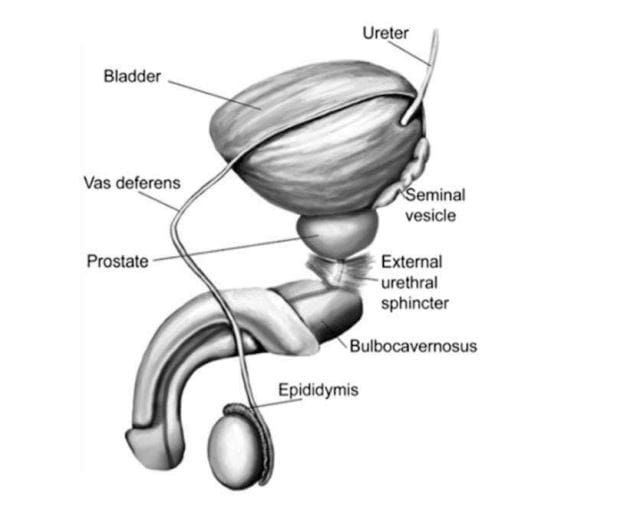
Image @CICS
Is controlled by the central nervous system. It has two phases.
- The vas deferens contracts pushing sperm to the base of the penis. The prostate gland and seminal vesicles release secretions to make semen.
- The muscles at the base of the penis begin to contract forcing semen out of the penis.
Ejaculation can be held back by learning to ‘edge’. This can be done through implementing a pause in stimulation, controlled breathing, mindfulness, and using fingers to squeeze either the base of the head of the penis at the frenulum, or the base of the penis.
Ejaculations can become weaker with less semen with age.
Some cultures have a belief that semen is a very potent source of energy, and that ejaculation results in a loss of ‘life force energy’. The older the male, the longer the periods of time between ejaculation should be observed. Sexual stimulation with orgasm and without ejaculation is favoured.

Image @slimesunday
Orgasms can be independent from ejaculation. Often they are at the same time. A person with a penis can orgasm without ejaculating, and ejaculation can happen without having had an orgasm.
Thank you.

Lisa McGarva -Clinical Sexologist, Relationship Therapist, Counsellor, Yoga Teacher, Yoga Therapist and Educator. Lisa is the founder of Thinking Feeling Moving, an online global Private Practice where clients can access better health in their mind, body, and in their relationships. Online sessions available globally, you may make a booking through the website https://www.thinkingfeelingmoving.com
Clinical Sexology + Relationship Therapy + Counselling. Thinking Feeling Moving is a LGBTQIA+ friendly safe space, GSRD aware and sex positive. Lisa is pluralistic in her approach drawing on many theories and techniques to best suit the client’s needs.
Yoga Therapy sessions. Are programmes which are individually designed for clients. After a consultation, Lisa creates a specialised filmed yoga class just for you. This class can be downloaded to your device. The programme is updated as your body heals and comes back into balance. Yoga Therapy is an intensive individualised programme to bring your body back into balance in recovering from illness, injury, surgery or if you are requiring a practice and have high needs with your body. Lisa is a 500hour trained Yoga Teacher (Yoga Australia), and Certified Yoga Therapist (International Association of Yoga Therapists). Private Yoga Classes are also available online.
Reconnection Retreat. Awaken and expand your sexuality and intimacy possibilities.
A tailored package designed just for you, offering a holistic approach of Clinical Sexology, Relationship Therapy and Yoga Therapy. Elevate your sex life and enrich your relationship/s. This package is for clients who wish to attend Therapy in a concentrated amount of time. Immerse yourself in healing and pleasure, combining it with your time off. A chance to really get away and attend to what is important to your life. Lisa can meet you globally as your personal Therapist at a negotiated destination.
Lisa’s YouTube channel is a space for deep rest where you can find dozens of guided Yoga Nidra Meditations filmed in beautiful places around the world. Access deep rest for your body and mind anytime on your device. Lisa also hosts many interviews with prominent leaders in the areas of Sexology, and Yoga Therapy.
She is global calling a few different continents home which is why she works primarily online. She loves travelling with her Husband who is a fellow explorer in travels, experiences and love.